Sandtray and Sandplay in the Treatment of Trauma with Children and Adolescents: A Systemic Review
Nerea Benito Herce
University of the Basque Country (UPV/EHU)
Iñigo Ochoa de Alda
University of the Basque Country (UPV/EHU)
José Luis Gonzalo Marrodán
Lotura Psychology and Traumatherapy Center
There are no known conflicts of interest to disclose.
Correspondence concerning this article should be addressed to Nerea Benito, nerea.benito4@gmail.com
https://doi.org/10.58997/wjstp.v2i1.74
Abstract
Experiencing a traumatic event during a developmental stage, such as childhood and adolescence, is related to an increased risk of physical and mental health problems during the rest of life. Given the high prevalence of traumatic experiences in childhood, there is a need for techniques such as Sandplay, which allows working with trauma in a way that is adapted to these children. The objective of this review is to compile the existing evidence on the efficacy of Sandplay Therapy (ST) in the treatment of trauma in children and adolescents. The results show a significant effect of ST on post-traumatic, internalizing, and externalizing symptoms, as well as on adolescents' adherence to therapy and on the well-being of children who have suffered collective traumatization (natural disasters, bombings, etc.). Although the studies in this review show encouraging evidence, there is a lack of studies, and it is necessary to subject Sandplay Therapy to more research with different populations and contexts. This way, the benefit that this tool can bring to the treatment of childhood trauma in the field of clinical psychology and child protection services will be confirmed.
Keywords:Childhood trauma, sandtray, sandplay, children and teenagers, efficacy, treatment
Childhood trauma affects a significant number of people worldwide. According to the World Health Organization (WHO), more than a third of the general population has experienced adverse, potentially traumatic experiences during childhood (Kessler et al., 2010). In fact, it is estimated that three hundred million children aged 2 to 4 years suffer from situations of violence at the hands of their caregivers (Olaguibel, n.d.). In summary, a study by McLaughlin et al. (2013) estimates that over 60% of minors will have experienced a potentially traumatic event by the end of adolescence.
Trauma is described as an experience that involves a perceived threat of death or physical harm and can generate feelings of fear, terror, and helplessness. This experience can occur in isolation or through continuous and chronic exposure to the threat. Traumatic experiences include abuse, violence, neglect, loss, accidents, natural disasters, wars, and other harmful experiences (APA, 2000). According to the DSM-5 (APA, 2013), trauma and stress-related disorders can manifest through highly variable symptoms grouped into three syndromes: re-experiencing, overactivation, or heightened arousal and cognitive alterations. Exposure to a traumatic event can generate symptoms related to fear and anxiety or symptoms of anhedonia and dysphoria (APA, 2013).
In a stage like childhood and adolescence, experiencing trauma significantly impacts development. According to Edwards et al. (2003), experiencing trauma in childhood is associated with a higher risk of developing physical and psychological problems. These negative effects can persist into adulthood. Exposure to traumatic experiences in childhood is linked to a higher risk of developing multiple disorders, such as attention deficit hyperactivity disorder (ADHD), depression, anxiety, and personality disorders. It can even profoundly affect a person's cognitive, social, and emotional capacities (Dye, 2018).
Therapy with children who have experienced trauma is more complex than with adults. Some children may not yet fully mastered language and may have more difficulty than adults in verbalizing their experiences. Therefore, it is important to have specific techniques that allow children to work with traumatic content in a way that is adapted to them and their developmental stage. One of the most common interventions in child therapy is play therapy. Play-based therapy helps children evolve into more adaptive behavior, healing their emotional wounds through play (Han et al., 2017). The child's world is accessed by including play in therapy, and they are provided with an appropriate means of expression. Due to its playful and child-adapted nature, a psychotherapeutic technique used recently with traumatized children is the sand tray. The sand tray technique was created by Margaret Lowenfeld (1935/1939) and developed by Dora Kalff. In her work with children, Margaret Lowenfeld discovered that she could better connect with them emotionally through objects and a sand tray without the need for words. She called her technique "the technique of worlds" (World Technique), and today, her method is known as Sandtray therapy (Lowenfeld, 1935, 1939). Subsequently, Dora Kalff became interested in Lowenfeld's work and added the idea that these representations of children in the tray corresponded to the individuation processes described by Carl G. Jung (Kalff, 2003). Based on Carl G. Jung's theory of the self, Kalff developed her own method of working with the sand tray, ST (Sandplay Therapy). Throughout this work, references to the sand tray will refer to Dora Kalff's method, Sandplay Therapy, and will be abbreviated as ST.
In therapy, the sand tray should have dimensions of 72 x 57 x 8 cm, allowing both the therapist and the patient to observe the entire tray in their field of vision (Kalff, 2003). The spatial boundaries of the tray act as a regulatory and protective factor, as they maintain the representation that the patient is externalizing within a limited space (Kalff, 2003). This is one of the reasons why the therapist never manipulates anything inside the tray, as it is considered to contain part of the patient's psyche (Homeyer & Sweeney, 1998).
Some general guidelines should be followed when creating a sand tray according to Kalff's method (Sandplay therapy). The patient should be positioned in front of a shelf filled with figures that represent as best as possible everything existing in the real world and even in fantasy: trees, people with different characteristics, fantasy characters, villains, heroes, means of transport, furniture, animals, and more. The therapist invites the patient to use these items to represent in the tray some aspect of their psychological state, either in the present or the past, chosen freely by the patient. While providing guidance, the therapist should let the patient choose the figures that particularly catch their attention or are significant to them (Kalff, 2003). The child places the figures in the sand, representing parts of their psyche. According to Kalff (2003), the patient will externalize a conflict from their inner world and bring it into the sand tray. With children, through play and, optionally, a conversation about the scene, a transformation of the conflict is achieved. The child is processing what has happened or is happening in real life differently. In their sand world, patients also represent their emotional strengths, which should be of interest during the therapeutic process (Marrodán, 2013). It is essential in a healing process to see the patient as someone with resources and strengths that need to be enhanced. According to Marrodán (2013), we must identify the resilient aspects each patient expresses in their tray and help them recognize them.
Throughout the entire process, the therapist must maintain an open and non-directive attitude, therefore refraining from making judgments or interpretations about what the person creates (Roesler, 2019). Through listening and empathetic feedback, a free and protected space must be created (Kalff, 2003) where the child feels safe to express what they want and need. The therapist can hypothesize about the connection between what the child represents and real life. However, it is not necessary to verbalize these hypotheses because working in the symbolic realm, in that protected space, is already therapeutic (Kalff, 2003). If the therapist wishes to convey an observation verbally, it should always be expressed as a possibility that the patient can confirm or refute (Marrodán, 2013).
When evaluating the usefulness and suitability of a technique, attention should be paid to the existing empirical evidence regarding its effectiveness. In the case of ST, some studies have demonstrated its efficacy with children in the treatment of aggressive and externalizing behavior problems (Han et al., 2017), ADHD (Wang et al., 2012), social behavioral problems and low self-esteem (Sim & Jang, 2013), and more. Furthermore, its applicability has been demonstrated in different populations, such as children with autism spectrum disorder (Lu et al., 2010). ST is a technique applicable to groups, making it especially useful when many people need assistance and time resources are limited. In fact, a version of the technique developed by Pattis (2011) is applied in a group context and consists of 12 sessions, during which each participant creates their own sand tray. This version of the technique has been used in the treatment of vulnerable populations, such as children who are victims of collective trauma (Roesler, 2019). ST has also been applied in a group format to survivors of an earthquake in Nepal (Hwang & Kim, 2017), victims of a tsunami (Lacroix et al., 2007), and individuals who have gone through a migration process (Jang & Kim, 2012).
As mentioned earlier, childhood trauma has a powerful and lasting impact on children. When working with traumatized children, it is necessary to adapt to them by providing a means of expression that protects them from potential re-experiencing of the trauma. Recent research indicates that trauma is embedded in implicit memory (Schore, 2001), subcortical brain structures (Perry, 2009; Van der Kolk, 2002;), and in the body (Van der Kolk et al., 2012), remaining outside of consciousness. Working with this unconscious content through narration can retraumatize the person (Marrodán, 2013). Therefore, ST is an especially useful technique because it allows the patient to express their inner world through symbols without the need for words, preventing re-traumatization (Roesler, 2019). Moreover, ST enables children who have suffered trauma to develop a sense of control, something they did not have during the traumatic event (Marrodán, 2013). In this world, they can do something they could not do when they experienced the trauma, or they can see represented what they wished had happened.
On the other hand, through contact with the sand and self-regulation with the therapist's assistance, ST allows the sensory impact of trauma to be addressed. Thus, it is possible to integrate the emotional and implicit aspects with the explicit, narrative, or verbal content of the event (Marrodán, 2013). In this regard, Freedle et al. (2015) highlight four strengths of ST in the treatment of trauma: relational safety, multi-sensory processing, expression of the traumatic narrative through symbols, and facilitation of the healing response of the self. Recent neuroscientific research suggests that ST not only heals traumatic experiences at a psychological level but also at a neurobiological level (Freedle et al., 2015).
For all the reasons mentioned above, ST is a useful and appropriate technique for the treatment of children who have experienced trauma. However, because it is an expressive and highly personal technique, it is difficult to assess and quantify the results of a ST process. One of the first steps in facilitating the evaluation and scientific research of this tool is the contribution of Mitchell and Friedmann (1994). These authors developed a method for analyzing the stories created in the tray. Their research found that during the healing process, patients express two main themes in their sand trays: wounding and healing themes. Those who have experienced trauma and are in the early stages of therapy more frequently represent wounding themes. In contrast, those who do not have a traumatic history or are in more advanced stages of therapy tend to represent healing themes (Yeh et al., 2015). Both wounding themes and healing themes evolve throughout ST therapy, not only in terms of frequency but also in the way they are represented.
Taking into consideration the high prevalence of potentially traumatic events in childhood and the short- and long-term consequences they generate, there is an evident need for appropriate and empirically validated techniques for therapy with these children. Due to its non-verbal nature and playful character, ST seems to be a very suitable technique for this purpose. Consequently, this work aims to compile existing evidence on the effectiveness of Sandplay therapy with children and adolescents who have experienced trauma. Specifically, it focuses on conducting a systematic review of ST's effectiveness in treating childhood traumas in children and adolescents.
Methodology
Bibliographic Search Strategy
To conduct a systematic search on the effectiveness of Sandplay Therapy (ST) in the treatment of childhood traumas with children and adolescents, electronic databases including Scopus, Web of Science, and Psychinfo were consulted.
In this search, the terms "Sandplay" and "Sandtray" were used, combined with the operator OR, and "childhood trauma" combined with the operator AND. Although the method under study in this work is Dora Kalff's ST, articles with the term "Sandtray" were also included in the search so as not to overlook important studies. This is because the nominal differentiation between these two techniques is not clearly and rigorously made in current scientific research (Wiersma et al., 2022). The search was conducted between March and April 2022, and the resulting studies were limited to academic articles published in the last 10 years in English and Spanish. After reviewing the results, a decision was made to conduct a second search due to the lack of articles that met the objective of this work and noting references to relevant studies from previous years in recent research. In this second search, articles published between 2009 and 2012 were included. Therefore, the final search included articles published in the last 13 years.
Article Selection
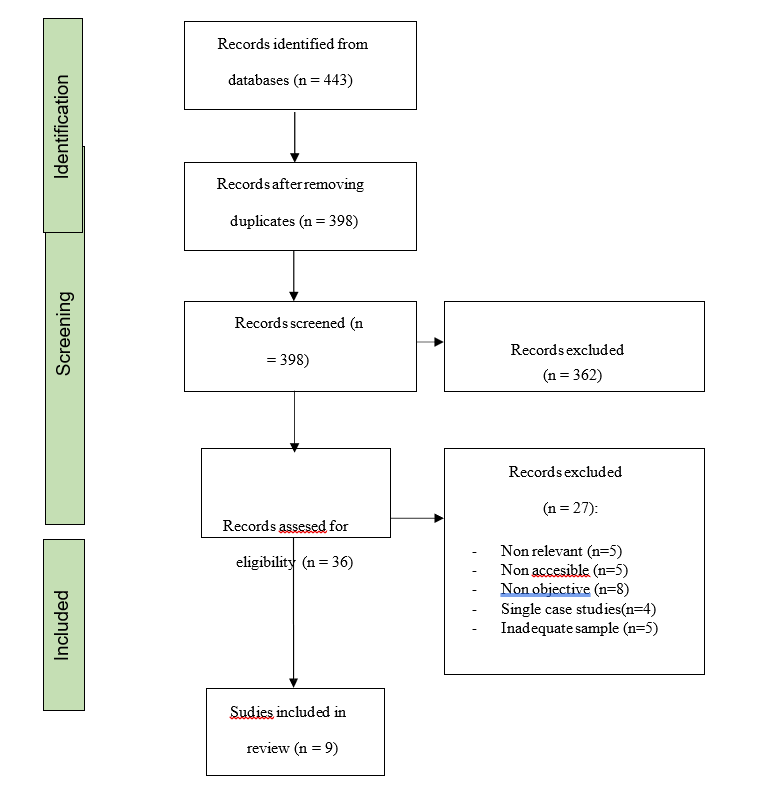
The article selection process was carried out following the guidelines of the PRISMA method (Moher et al., 2009). In the first identification phase, the two searches conducted yielded 443 articles. After eliminating duplicates, the total number of articles obtained in the search was reduced to 398.
In a second screening phase, the titles and abstracts of all articles were reviewed. Only those that followed these criteria were selected: 1) conducted research with an experimental quantitative and/or qualitative design and 2) whose primary purpose was to analyze the effectiveness of the sand tray in the treatment of children who have experienced trauma. Additionally, articles were excluded if they 1) primarily explained the symbolism of an object in the sand tray, 2) dealt with clinical populations of children with other pathologies such as ADHD, obesity, etc., 3) compared the sand tray with other techniques descriptively, or 4) were single-case studies.
In the review of titles and abstracts, 362 articles out of the initial 398 were discarded, leaving 36 articles for full-text analysis. In the eligibility phase, 27 articles were further excluded for not being relevant to the study (n=5), not being accessible in any of the reviewed databases (n=5), not fitting the study's objective correctly (mentioning trauma only superficially) (n=8), containing an inadequate sample (n=5), or being single-case studies (n=4). Therefore, the final review includes 9 articles. Figure 1 illustrates the flowchart of the article search and selection process. (See Appendix 1.)
Results
ST In Treatment with Children Who Have Suffered Trauma
Over the years, different authors have been interested in verifying the effectiveness of Sandplay Therapy (ST) in the treatment of children who have experienced trauma. Specifically, in 2010, Von Gontard et al. (2010) examined the effectiveness of ST in 56 children aged 5 to 18 who exhibited internalizing and externalizing symptoms. The authors did not include the trauma history of the children as a variable, but they did use a clinical sample of participants diagnosed with one or more disorders. This study is noteworthy because the symptoms exhibited by the participants are often seen in those who have experienced trauma. Symptomatic data was collected using the Child Behavior Checklist (CBCL; Achenbach, 1991). Comparing the initial scores with those six months after starting ST, a statistically significant reduction in symptoms of withdrawal, somatic symptoms, anxious-depressive symptoms, attentional problems, aggression, thought disturbances, internalizing problems, and behavioral problems were observed (Von Gontard et al., 2010). However, in comparing scores six months after and twelve months after starting treatment, only the reduction in attentional symptoms, aggression, internalizing symptoms, and behavioral problems was statistically significant (Von Gontard et al., 2010). Consequently, the authors suggest that with some children, 6 months of ST may be sufficient to observe a significant change. After a year, the authors observed a significant change in all CBCL scales (Von Gontard et al., 2010).
A recent study conducted by Matta and Ramos (2021) evaluated the effectiveness of ST with minors who were victims of abuse and exhibited internalizing and externalizing behavioral problems. The sample consisted of 60 children aged 6 to 10, divided into a control, experimental, and placebo group. To measure their behavior and level of symptomatology, the authors also used the Child Behavior Checklist (CBCL; Achenbach, 1991). After ST sessions, the results showed a significant reduction in internalizing and externalizing symptoms in the experimental group, both showing a large effect size. Additionally, they found that the proportion of negative scenarios in the sand trays was much lower in the last ten therapy sessions. A significant increase in positive scenarios was found in the second half of therapy. This study concludes that brief ST can effectively reduce internalizing and externalizing behavioral problems in children aged 6 to 10, and this effect persists for up to six months after the intervention. Working with minors who have experienced abuse using a technique like ST can promote changes in self-regulation and in their symptoms. Additionally, it may help prevent potential consequences of abuse that may appear in adulthood, such as depression or chronic patterns of disorganization (Matta & Ramos, 2021).
On the other hand, Rousseau et al. (2009) applied individual ST to 105 children aged 4 to 6 residing in a multi-ethnic neighborhood with a history of migration. Many of the participating families in the study reported having experienced organized violence in their places of origin (either witnessing violence or being persecuted). Furthermore, at the time of the study, a tsunami struck South Asia, the place of origin for many of the children in the sample. Their concern for their families and interaction with their parents, who were also concerned, may have influenced their situation and made it worse than that of other children. Data was collected through interviews with parents and teachers, who responded to the Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001). After applying ST, parents' information indicated a significant reduction in the total SDQ score, as well as in emotional symptoms and in the relational subscale. These differences were not observed in the control group. Teacher-reported information indicated that emotional and behavioral symptoms did not decrease in the experimental group but increased significantly in the control group. One possible explanation is that ST intervention in the experimental group prevented the increase of symptoms that the tsunami generated in the control group. No differences were found in the level of symptoms between children whose families had experienced violence during the migration process and the rest of the children in the sample. However, the program was much more effective in children who had experienced such violence. The authors noted that the children represented the tsunami and the traumatic experiences their families had suffered in their sand trays. Their experience with this technique also allowed them to process their indirect exposure to trauma. The study concludes that ST can have a positive effect on preschool-aged children who have directly or intergenerationally experienced adversity (Rousseau et al., 2009).
Recent research suggests that ST can be a useful tool not only for treating trauma but also for identifying it. Tornero and Capella (2017) observed the process of ST in seven children aged 7 to 10 who had experienced sexual abuse. They found that most of the children dug and hid objects in the sand tray, representing the secrecy that accompanies sexual abuse. Other studies have also observed this behavior (Homeyer & Landreth, 1998), although the authors emphasize that the meaning each child assigns to this action should be analyzed individually. The play of these children at the beginning of therapy is very chaotic, and there are some objects they choose very frequently, such as snakes, symbolizing constant fear induction and the harm caused by abuse (Tornero & Capella, 2017). Although this area requires further research, it appears that many children represent their abuse experiences, similarly, using the same symbols and displaying a similar behavioral repertoire.
ST In Treatment with Adolescents Who Have Suffered Trauma
ST is a technique particularly suitable for psychotherapy with adolescents who have experienced trauma. During adolescence, those who have suffered trauma in their childhood are at a higher risk of developing addictions and various mental health disorders. For example, several studies indicate an existing relationship between a history of trauma and substance abuse problems (Blumenthal et al., 2008; Bujarski et al., 2012). When these two issues occur together, it's essential to ensure that the treatment can address both. Although cognitive-behavioral therapy has proven effective for substance abuse problems, adolescents who have experienced trauma often tend to drop out of this type of treatment (Freedle et al., 2015). Therefore, an additional intervention focused on trauma is needed to increase their adherence to therapy.
A recent study evaluates the effectiveness of including expressive therapies like ST in the treatment of adolescents with a substance abuse disorder and a history of trauma (Freedle et al., 2015). Adolescents participating in this recovery program, including ST, show improvements in their daily functioning at home, school, and the community. After 16 weeks of treatment, the severity of their substance abuse problem also decreases, as well as their trauma-related distress (Freedle et al., 2015). Adolescents and therapists in the program highlight ST is useful to express all the pain that trauma continues to cause them. These adolescents turn to addiction in an attempt to self-regulate. Offering them a process like ST can be an alternative way to calm their nervous system and externalize all the internal content of the trauma (Freedle et al., 2015). Including ST in treatment programs for vulnerable adolescents appears to offer multiple benefits, especially in the case of adolescents dealing with both substance abuse issues and a history of trauma, as it reduces the rate of therapy dropouts.
As mentioned earlier, ST appears to be a useful technique both for the treatment and for the identification of trauma in children. A recent study has tested ST as a technique for identifying signs of psychological trauma in unaccompanied adolescents in the Netherlands (Dobretsova & Batista, 2019). These teenagers create chaotic and disorganized scenarios in their sand trays. Many of their stories incorporate the "wounding themes" described by Mitchell and Friedman (1994). Additionally, consistent with other studies, the authors find that reluctance to interact with the sand can be another indicator of psychological trauma (Shaia, 1991). The fact that the adolescent remains silent and does not describe their world in the sand, perhaps because it is too painful, is also hypothesized as a possible sign of trauma. Although this needs further study, there are some indicators represented in the sand trays by most adolescents who have experienced abuse or trauma in childhood. Therefore, ST can be a method for identifying childhood trauma in the case of adolescents (Dobretsova & Batista, 2019).
ST In Moments Of Social Crisis and Natural Disasters
Much of the current research on Sandplay Therapy (ST) has been focused on treating children exposed to a traumatic social event, such as war, a terrorist attack, an earthquake, or a volcanic eruption. As Freedle et al. (2021) point out, children are particularly vulnerable to developing post-traumatic stress disorder (PTSD) after exposure to a natural disaster or an impactful event. They may be more affected by these types of events because they haven't yet reached a sufficient level of maturity, and they rely on the support of adults who have also experienced trauma (Wang & You, 2022). The distress they experience in response to these events affects them physically, emotionally, behaviorally, socially, and academically. Therefore, providing quality psychological treatment in early stages is crucial.
Children from low socioeconomic status families are especially vulnerable to developing PTSD (Freedle, 2021). They are also the ones with less accessibility to psychological therapy due to economic constraints. Thus, it is important to have a technique like ST that can be applied in group settings and in a school context. This way, it is possible to reach children who have experienced trauma and are at risk of developing PTSD. The non-verbal nature of the technique allows for working and forming a connection with all children, regardless of their cultural background and language proficiency (Yeh et al., 2015). Therefore, it is a highly suitable technique for the multicultural environment in schools today.
Additionally, applying ST in a group setting offers even more emotional and social benefits, allowing them to share a space with their peers (Freedle et al., 2021). According to their teachers, conducting ST in this format improves the cohesion of the children as a group (Freedle et al., 2021). For all these reasons, one of the recent research objectives regarding ST has been to test its effectiveness when applied to groups of children in a school context.
Yeh et al. (2015) applied ST to 32 children affected by the terrorist attack on the World Trade Center in the United States. The researchers considered ST suitable for therapeutic work in schools because it allows for working with those who do not have a strong command of English and with children whose culture does not align well with traditional talk therapy. The results of this study show that, after receiving group ST, children significantly improved academically, psychologically, and behaviorally. The therapy positively impacted their English and Math scores, the assessments made by teachers and therapists regarding their behavior, and even their school attendance (Yeh et al., 2015). Conducting ST with a group of children seems to improve not only their mental health and emotional well-being but also their behavior, learning, and cognitive development (Mitchell & Friedman, 1994; Russo et al., 2006; Yeh et al., 2015). In line with what Mitchell and Friedmann (1994) noted about Wounding and Healing themes, children represented many stories with wounding themes in their sandboxes due to their recent traumatic experiences. However, these themes evolved, and researchers observed a positive change in the representations in the sand tray. The authors highlight ST as a suitable technique for therapy during times of crisis and coping with a traumatic event (Yeh et al., 2015).
In 2021, Freedle et al. conducted therapeutic work with ST involving 12 children aged 6 and 7 who had lost their school and, in many cases, their homes due to the eruption of the Kilauea volcano in Hawaii. These authors evaluated the level of anxiety and post-traumatic symptoms in the children before and after the intervention. The results showed a significant reduction in anxiety symptoms and post-traumatic symptoms, with a large effect size in both cases (d = 1.25 and d = 1.40, respectively). Sleep-related symptoms improved in half of the children and did not worsen in the rest. Regarding Mitchell and Friedman's (1994) wounding and healing themes, there was a reduction in wounding themes as therapy progressed, with an increasing presence of healing themes. The authors suggest that this pattern may signify a shift in the psyche toward greater organization, congruence, and integrity (Freedle et al., 2021).
Moreover, teachers reported in an interview that they observed improvements in the children's behavior, academic performance, and well-being. They also noted that the experience with ST encouraged these children to talk to their parents about their concerns regarding the event. The results of this study provide further evidence of the positive effect of ST on coping with traumatic events in children. ST is a technique that helps children share their stories, access their unconscious resources, alleviate psychological distress symptoms, and promote resilience (Chenghou & Shen, 2010; Freedle et al., 2021; Kawai, 2015; Lacroix et al., 2007; Lee & Jang, 2020; Park, 2018; Zoja, 2011).
Wang and You (2022) applied ST to 96 children aged 6 to 18 who had experienced the Wenchuan earthquake. They found that, after an initial improvement, these children worsened again 12 months after the natural disaster. However, they observed another improvement later, as children began to represent more healing themes and fewer wounding themes in their sand trays. The authors suggested paying particular attention to what happens one year after the traumatic event, as this is when children start dealing with it on their own and may be particularly affected. At this point, the sand tray can be a useful tool for treating and preventing worsening symptoms. These authors propose treatment in four phases: accommodation (up to 6 months after the event), connection with the children (6-12 months), trust (12-24 months), separation, and freedom (after 24 months) (Wang & You, 2022). Tables 1, 2, and 3 display the results and main characteristics of the studies obtained in the search (see Appendix 2).
Discussion and Conclusions
This review aimed to compile existing evidence on the efficacy of the Sandtray in the treatment of children and adolescents who have suffered trauma.
In the case of children, ST appears to be effective not only in the treatment of internalizing symptoms but also in the treatment of externalizing symptoms (Matta & Ramos, 2021; Von Gontard et al., 2010). These results are in congruence with those obtained by Han et al. (2017), who apply ST to ten 4- and 5-year-old children with externalizing behavior problems and compare the results with those of a control group not receiving treatment. In this study, it is concluded that ST offers these children the possibility of expressing their contained emotions, thus reducing their levels of aggression. ST offers an alternative way to express the feelings and difficulties that cause disruptive behavior. Another study by Kwak et al. (2020), which applies ST in group format to 284 children, also finds that the technique has a significant effect on both emotional symptoms (tension/anxiety, phobia, sleep difficulties...) and behavioral symptoms (inattention, behavioral problems...). Therefore, recent research seems to indicate that ST may be an appropriate technique with those children who show internalizing symptoms (withdrawal, sadness...) but also with those who tend to externalize their difficulties (disruptive behavior, hyperactivity...).
As mentioned above, suffering trauma in childhood affects children's development and increases the risk of developing numerous disorders such as ADHD, depression, anxiety, etc. In other words, we know that in these children, the consequences of trauma can appear both in childhood and in later adulthood through internalizing or externalizing symptomatology. Consequently, ST seems to be a very appropriate technique for the treatment of these children since it significantly improves both types of symptoms (Han et al., 2016; Kwak et al., 2020; Matta & Ramos, 2021; Von Gontard et al., 2010) and protects them from the re-traumatization caused by the creating a narrative of the trauma (Marrodán, 2013).
On the other hand, studies in this review agree that ST can be a helpful tool not only for therapeutic work but also for the analysis and identification of trauma. Qualitative observations indicate that those who have suffered trauma tend to express similar behavioral repertoires when doing the sandplay. For example, they tend to hide objects more frequently (Tornero and Capella, 2017) and interact less with sand (Dobretsova & Batista, 2019; Shaia, 1991). Additionally, both children and adolescents who have experienced trauma create very chaotic scenarios and play in a very disorganized manner in the early stages of therapy (Dobretsova & Batista, 2019; Tornero & Capella, 2017). As discussed in the introduction, children begin their process by representing wounding themes and evolve to more frequently represent healing themes (Dobretsova & Batista, 2019; Freedle et al., 2021; Matta & Ramos, 2021; Wang & You, 2022; Yeh et al., 2015). Although it is something that still requires much research, children who have experienced trauma seem to represent their own trauma in the sandplay in a similar way. A future line of research with ST maybe its possible diagnostic value, creating a more specific coding system that facilitates the observation and analysis of the sessions. Establishing which behaviors are repeated in the sandplay of these children would facilitate the identification of situations of abuse, mistreatment, or trauma. Therefore, allowing therapists to more clearly identify when a child is at risk of living or having lived a traumatic situation.
Regarding adolescents, the articles found in the review are very few and highlight the need for further research in this field. Due to their stage of development, one of the significant challenges in therapy with adolescents is their adherence to therapy. The study by Freedle et al. (2015) indicates that ST, in addition to reducing the severity of substance abuse and distress symptoms, can increase adolescents' adherence to the program. According to Parker and Cade (2018), a possible explanation is that ST offers a choice to the patient as he/she decides him/herself what to do with the sandplay and the figurines. This allows a more empathic relationship with the patient and promotes a greater desire for collaboration on his/her part (Parker & Cade, 2018). Many adolescents who have suffered trauma come to therapy obliged by external figures. Consequently, their motivation and collaboration in the process may be compromised. Thus, clarifying whether including ST, a trauma-sensitive technique, in the therapeutic process also promotes adherence may be of great interest.
Studies indicate that ST is also an appropriate technique for dealing with children in crisis situations such as bombings, natural disasters, or war situations. It reduces post-traumatic and externalizing symptoms, and teachers report that children improve their academic performance, general well-being, and classroom behavior after ST sessions (Freedle et al., 2021; Yeh et al., 2015). At the time of this review, a war in Ukraine is causing traumatic experiences of varying degrees in the children of that country; a traumatic damage that, with further study and according to the data acquired so far, could be assessed and treated using a technique such as ST.
Although, in recent years, there has been increasing interest in proving its efficacy through empirically validated studies, there is still a need for further research on this technique in an experimental context. In fact, since Dora Kalff presented her method of ST in 1996, most of the studies published about this technique have been elaborated in a single-case format (Von Gontard et al., 2010). Of all the articles screened in this review, many of them are single cases. Consequently, it can be hypothesized that many psychotherapists find sufficiently remarkable cases in their clinical practice that they later publish. However, the research field has not yet paid enough attention to this technique. This case is one more example of an issue in the research field of psychology. There are techniques that clinicians find effective in their practice but have not yet been analyzed by large-scale studies to prove their efficacy.
Nevertheless, it is also true that ST is a difficult technique to submit to currently established standards of scientific evidence. It is challenging to conduct ST studies with a large sample, as it requires a large amount of material and time resources with each patient, even though it can be applied in a group setting. Additionally, each ST process is different, and each person benefits from his or her own experience with sandplay, which is different from that of others. Therefore, it is not easy to establish the underlying mechanisms of change common to all ST processes. Although Mitchell and Friedmann (1994) took a first step by categorizing wounding and healing themes, this area still requires further research.
Among the limitations of this review is the small sample size of most of the studies. In general, there is a lack of quantitative and large-sample studies on ST in the treatment of childhood trauma. The articles found in this search show certain progress since they explain its curative effect and possible diagnostic value. However, all the authors agree that more research is needed since many of their studies do not have a sufficiently large sample or have become obsolete due to the passage of time. In many articles, reference is made to valid studies carried out in previous years. These investigations should be replicated to observe whether the benefit with current populations is still the same.
As mentioned in the introduction, childhood traumatic experiences affect many people in the world. Because of their great and lasting impact on those who suffer from them, it should be in the best interest of society to protect all these children from their consequences. In the work with children, treating the consequences of trauma becomes even more challenging for two main reasons. On the one hand, many of them have not developed the capacity to express their experiences through language while maintaining sufficient emotional regulation. On the other hand, therapy at this stage of life requires techniques specifically adapted to the stage of development. The use of ST is especially useful in the treatment of childhood trauma because it can incorporate play, which is attractive to children and non-threatening, and because it does not require the elaboration of the traumatic contents through language. For this reason, it seems important to validate a technique such as ST, adapted to the characteristics of the child population, sensitive to traumatic damage, and protective against possible re-traumatization.
All in all, the review shows encouraging evidence but also indicates that it is still necessary to subject ST to more studies with different populations and in other contexts to confirm the benefit that this technique can bring to the treatment of child trauma in the field of clinical psychology and child protection services.
References
Achenbach, T. M., & Rescorla, M. A. (2001). Manual for the ASEBA School-age forms & profiles. University of Vermont.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., Text rev.). American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Blumenthal, H., Blanchard, L., Feldner, M. T., Babson, K. A., Leen-Feldner, E. W., & Dixon, L. (2008). Traumatic event exposure, post-traumatic stress, and substance use among youth: A critical review of the empirical literature. Current Psychiatry Reviews, 4(4), 228-254. https://doi.org/10.2174/157340008786576562
Bujarski, S. J., Feldner, M. T., Lewis, S. F., Babson, K. A., Trainor, C. D., Leen-Feldner, E., … & Bonn-Miller, M. O. (2012). Marijuana use among traumatic event-exposed adolescents: Post-traumatic stress symptom frequency predicts coping motivations for use. Addictive Behaviors, 37(1), 53-59. https://doi.org/10.1016/j.addbeh.2011.08.009
Chenghou, C., & Shen, H. (2010). "Garden of the Heart-Soul" in the Earthquake Area of China: Creativity and Transformation. Jung Journal: Culture & Psyche, 4(2), 5-15. https://doi.org/10.1525/jung.2010.4.2.5
Dye, H. (2018). The impact and long-term effects of childhood trauma. Journal of Human Behavior in the Social Environment, 28(3), 381-392. https://doi.org/10.1080/10911359.2018.1435328
Dobretsova, A., & Batista, E. (2019). Sandplay: Psychotrauma signs in asylum seeking adolescents. Journal of Infant, Child, and Adolescent Psychotherapy, 18(4), 403-416. https://doi.org/10.1080/15289168.2019.1583055
Edwards, V., Holden, G., Felitti, V., & Anda, R. (2003). Relationship between multiple forms of childhood maltreatment and adult mental health in community respondents: Results from the adverse childhood experiences study. The American Journal of Psychiatry, 160(8), 1453–1460. https://doi.org/10.1176/appi.ajp.160.8.1453
Freedle, L. R., Altschul, D. B., & Freedle, A. (2015). The role of sandplay therapy in the treatment of adolescents and young adults with co-occurring substance use disorders and trauma. Journal of Sandplay Therapy, 24(2), 127-145.
Freedle, L. R., McGee, M., Blenchman, S., Souza Jr, J. & Zandbergen, D. L. (2021). "The lava ate my school": The use of group sandplay to reduce anxiety and post-traumatic stress in displaced elementary school students. Journal of Sandplay Therapy, 30(2), 129-147.
Goodman, R. (2001). Psychometric properties of the strengths and difficulties questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 40(11), 1337-1345. https://doi.org/10.1097/00004583-200111000-00015
Han, Y., Lee, Y., & Suh, J.H. (2017). Effects of a sandplay therapy program at a childcare center on children with externalizing behavioral problems. The Arts in Psychotherapy, 52, 24–31. https://doi.org/10.1016/j.aip.2016.09.008
Homeyer, L. E., & Landreth, G. L (1998). Play therapy behaviors of sexually abused children. International Journal of Play Therapy, 7(1), 49. https://doi.org/10.1037/h0089418
Homeyer, L. E. & Sweeney, D. S. (1998). Sandtray: A practical manual (2ª edición). Routledge.
Hwang, H., & Kim, H. (2017). Effectiveness of sandplay therapy on earthquake survivors in Nepal. In Presentation at the International Society of Sandplay Therapy Congress.
Jang, M. & Kim, Y. H. (2012). The effect of group sandplay therapy on the social anxiety, loneliness and self-expression of the migrant women in international marriages in South Korea. The Arts in Psychotherapy, 39(1), 38-41. https://doi.org/10.1016/j.aip.2011.11.008
Kalff, D. M. (2003). Sandplay: A psychotherapeutic approach to the psyche. Temenos Press.
Kawai, T. (2015). Big stories and small stories in the psychological relief work after the earthquake disaster. In L. Huskinson & M. Stein (Eds.), Analytical Psychology in a Changing World: The search for self, identity and community. Routledge.
Kessler, R., McLaughlin, K., Green, J., Gruber, M., Sampson, N., Zaslavsky, A., . . . & Williams, D. (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. British Journal of Psychiatry, 197(5), 378-385. https://doi.org/10.1192/bjp.bp.110.080499
Kwak, H. J., Ahn, U. K., & Lim, M. H. (2020). The clinical effects of school sandplay group therapy on general children with a focus on Korea Child & Youth Personality Test. BMC psychology, 8(1), 1-6. https://doi.org/10.1186/s40359-020-0378-9
Lacroix, L., Rousseau, C., Gauthier, M. F., Singh, A., Giguère, N., & Lemzoudi, Y. (2007). Inmigrant and refugee preschoolers' sandplay representations of the tsunami. The Arts in Psychotherapy, 34(2), 99-113. https://doi.org/10.1016/j.aip.2006.09.006
Lee, S. & Jang, M. (2020). The effect of group sandplay therapy on psychological health and resilience of adolescent survivors of Nepal earthquake. Journal of Symbols & Sandplay Therapy, 11(2), 45-78. https://doi.org/10.12964/jsst.20007
Lowenfeld, M. (1935). Play in childhood. Victor Gollanz.
Lowenfeld, M. (1939). The world pictures of children. British Journal of Medical Psychology,18, 65–101. https://doi.org/10.1111/j.2044-8341.1939.tb00710.x
Lu, L., Peterson, F., Lacroix, L., & Rousseau, C. (2010). Stimulating creative play in children with autism through sandplay. The Arts in Psychotherapy, 37(1), 56–64. https://doi.org/10.1016/j.aip.2009.09.003
Marrodán, J. L. G. (2013). Construyendo puentes. Desclée de Brouwer.
Matta, R. M. D., & Ramos, D. G. (2021). The effectiveness of Sandplay Therapy in children who are victims of maltreatment with internalizing and externalizing behavior problems. Estudos de Psicología (Campinas), 38. https://doi.org/10.1590/1982-0275202138e200036
McLaughlin, K. A., Koenen, K. C., Hill, E. D., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., & Kessler, R. C. (2013). Trauma exposure and post-traumatic stress disorder in a national sample of adolescents. Journal of the American Academy of Child & AdolescentPsychiatry, 52(8),815-830. https://doi.org/10.1016/j.jaac.2013.05.011
Mitchell, R. R. & Friedman, H. S. (1994). Sandplay: Past, present, and future. Routledge.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G. & Prisma Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Annals of Internal Medicine, 151(4), 264–269. https://doi.org/10.1371/journal.pmed.1000097
Olaguibel, A. (n.d.). Cada 7 minutos muere un adolescente víctima de la violencia. UNICEF España. https://www.unicef.es/blog/violencia-infantil-una-realidad-demasiadas-veces-silenciada
Park, C.M. (2018). A study on the images used in sandplay therapy by children who experienced the Gyeongju earthquake. Journal of Symbols & Sandplay Therapy, 9(2), 27-48.
Parker, M. M., & Cade, R. (2018). Using sand tray therapy with juveniles in correctional settings. Journal of Addictions & Offender Counseling, 39(2), 78-88. https://doi.org/10.1002/jaoc.12048
Pattis, E. (2011). Sandplay therapy in vulnerable communities, a Jungian approach. Routledge. https://doi.org/10.4324/9780203817957
Perry, B. D. (2009). Examining child maltreatment through a neurodevelopmental lens: Clinical applications of the neurosequential model of therapeutics. Journal of Loss and Trauma, 14(4), 240-255. https://doi.org/10.1080/15325020903004350
Roesler, C. (2019). Sandplay therapy: An overview of theory, applications and evidence base. The Arts in Psychotherapy, 64, 84-94. https://doi.org/10.1016/j.aip.2019.04.001
Rousseau, C., Benoit, M., Lacroix, L. & Gauthier, M. F. (2009). Evaluation of a sandplay program for preschoolers in a multi-ethnic neighborhood. Journal of child psychology and psychiatry, 50(6), 743-750. https://doi.org/10.1111/j.1469- 7610.2008.02003.x
Russo, M., Vernam, J., & Wolbert, A. (2006). Sandplay and storytelling: Social constructivism and cognitive development in child counseling. The Arts in Psychotherapy, 33(3), 229-237. http://doi.org/10.1016/j.aip.2006.02.005
Schore, A. N. (2001). The effects of early relational trauma on right brain development, affect regulation, and infant mental health. Infant Mental Health Journal, 22(1-2), 201-269. https://doi.org/10.1002/1097-0355(200101/04)22:1%3C201::AID-IMHJ8%3E3.0.CO;2-9
Shaia, A. (1991). Images in the sand: The initial sand worlds of men molested as children (Tesis doctoral). California Institute of Integral Studies.
Sim, E., & Jang, M. (2013). Effects of sandplay therapy on aggression and brain waves of female juvenile delinquents. Journal of Symbols and Sandplay Therapy, 4(2), 45-50. http://doi.org/10.12964/jsst.130006
Tornero, M. D., & Capella, C. (2017). Change during psychotherapy through sand play tray in children that have been sexually abused. Frontiers in psychology, 8, 617. https://doi.org/10.3389/fpsyg.2017.00617
Van der Kolk, B. A. (2002). Postraumatic therapy in the age of neuroscience. Psychoanalytic Dialogues, 12(3), 381-392. https://doi.org/10.1080/10481881209348674
Van der Kolk, B. A., McFarlane, A. C., y Weisaeth, L. (Eds.) (2012). Traumatic stress: The effects of overwhelming experience on mind, body and society. Guilford Press.
Von Gontard, A., Löwen-Seifert, S., Watcher, U., Kumru, Z., Becker-Wördenweber, E., Hochadel, M., Schneider, S., Senges, C., & SAT Group. (2010). Sandplay therapy study: A prospective outcome study of sandplay therapy with children and adolescents. Journal of Sandplay Therapy, 19(2), 131-139.
Wang, Q. M., Hang, G., Zhang, X. L., He, X. L., & Wang, D. D. (2012). Effects of sandplay therapy in children with attention deficit hyperactivity disorder. Chinese Mental Health Journal, 24(9), 691-695.
Wang, D., & You, X. (2022). Post-disaster trauma and cultural healing in children and adolescents: Evidence from the Wenchuan earthquake. The Arts in Psychotherapy, 77, 101878. https://doi.org/10.1016/j.aip.2021.101878
Wiersma, J. K., Freedle, L. R., McRoberts, R., & Solberg, K. B. (2022). A meta-analysis of sandplay therapy treatment outcomes. International Journal of Play Therapy. https://doi.org/10.1037/pla0000180
Yeh, C. J., Aslan, S. M., Mendoza, V. E., & Tsukamoto, M. (2015). The Use of Sandplay Therapy in Urban Elementary Schools as a Crisis Response to the World Trade Center Attacks. Psychology Research, 5(7), 413-427. https://doi.org/10.17265/2159-5542/2015.07.004
Zoja, E.P. (2011). Sandplay therapy in vulnerable communities: A Jungian approach. Routledge.
Appendices:
Appendix 1: Flow diagram
Appendix 2: Summary of results after article selection.
Table 1. Main results of studies about ST in the treatment of children who have suffered trauma.
| Authors and year | Sample | Design and Methodology | General results |
|---|---|---|---|
| Rousseau et al., 2009 | 105 children aged 4-6 with a story of migration and/or violence:
|
Experimental quantitative and qualitative study with EG and CG. Pre and post treatment evaluation:
|
In EG, significant reduction of (according to parents):
|
| Von Gontard et al., 2010 | 56 children aged 5-18, diagnosed of internalizing externalizing or other disorders (CBCL):
|
Prospective non-randomized study. Pre and post treatment evaluation (0, 6, 12 months):
|
In the first 6 months of therapy, significant reduction of the following symptoms:
In the second half of therapy (6-12 months), significant reduction of the following symptoms:
|
| Tornero & Capella, 2017 | 7 children aged 7-10 who suffered child sexual abuse (CAVAS):
|
Longitudinal qualitative study.
|
Children:
|
| Matta & Ramos, 2021 | 60 children aged 6-10, who suffered maltreatment and live in welfare institutions in Sao Paulo:
|
Quantitative and qualitative experimental study, with EG, CG and PG. Pre and post treatment evaluation (0, 20 weeks, 6 months):
|
In EG, significant reduction of:
|
Nota. CAVAS: Centre of Attention to Sexual Abuse Victims in Chile, SDQ: Strenghts and Difficulties Questionnaire, CBCL: Child Behavior Checklist, EG: Experimental Group, CG: Control Group, PG: Placebo group.
Table 2. Main results of studies about ST in the treatment of adolescents who have suffered trauma.
| Authors and year | Sample | Design and Methodology | General results |
|---|---|---|---|
| Freedle et al., 2015 | 22 adolescents aged 14-24, diagnosed with SAD and with Trauma history (UCLA PTSD-RI y ACE Q):
|
Quasi-experimental study with qualitative and quantitative methods. Pre and post treatment evaluation (beginning, mid, ending):
|
BEAR program improves:
|
| Dobretsova & Batista, 2019 | 12 adolescents aged 15-17 and unaccompanied in The Netherlands diagnosed with TEPT (DSM-4-R):
|
Qualitative study:
|
The adolescents who suffered trauma:
|
Nota.SAD: Substance Abuse Disorder, UCLA PTSD-RI: UCLA Post Traumatic Stress Disorder-Reaction Index, ACE Q: Adverse Childhood Experience Questionnaire, CAFAS SU: Child and Adolescent Functional Scale, Y-OQ: Youth Outcome Questionnaire.
Table 3. Main results of studies about ST in situations of social crisis and natural disasters.
| Authors and year | Sample | Design and Methodology | General Results |
|---|---|---|---|
| Yeh et al., 2015 | 32 children aged 4-11, living in NYC and who suffered WTC's terrorist attack closely:
|
Study with qualitative and quantitative method. Pre and post treatment evaluation of:
|
Children improve in:
|
| Freedle et al., 2021 | 12 6-year-old children who suffered a volcano eruption:
|
Study with qualitative and quantitative method. Pre and post treatment evaluation:
|
Significant improvement in:
Representations in the ST:
|
| Wang & You, 2022 | 96 children aged 6-18 who suffered Wenchuan's earthquake. | Study with a qualitative method
|
|
Nota.WTC: World Trade Centre, RCMAS-2: Revised Children's Manifest Anxiety Scale- Second Edition, CROPS: Child Report of Post- Traumatic Symptoms, WT: Wounding themes, HT: Healing themes.
Original content from this work may be used under the terms of the https://creativecommons.org/licenses/by-nc-nd/4.0/. Any further distributions of this work (noncommercial only) must maintain attribution to the author(s), the title of the work, journal citation, and DOI.
© World Association of Sand Therapy Professionals, World Journal for Sand Therapy Practice, Volume 2, Number 1, 2024